About the research topic
Ultrasound is the preferred modality for image-guided ablation procedures in the liver. However, not all lesions are clearly visible in ultrasound, which is why CT-guided ablations are common as well. In this project, various segmentation and registration aproaches for improving image guidance as well as assessing ablation result, have been developed:
- a study on various vesselness filters for liver vessel segmentation ultrasound images,
- a registration approach for aligning pre-operative (diagnostic) images to post-operative images for treatment success assessment
- a registration approach for aligning pre-operative, contrast-enhanced diagnostic images to intra-operative (non-contrast-enhanced) images for improving image guidance
- an assessment of non-rigid deformation of the liver in these procedures
- a method and dataset for assessing Target Registration Errors (TRE) for contrast-enhanced liver CT to non-contrast-enhanced liver CT registration
Output
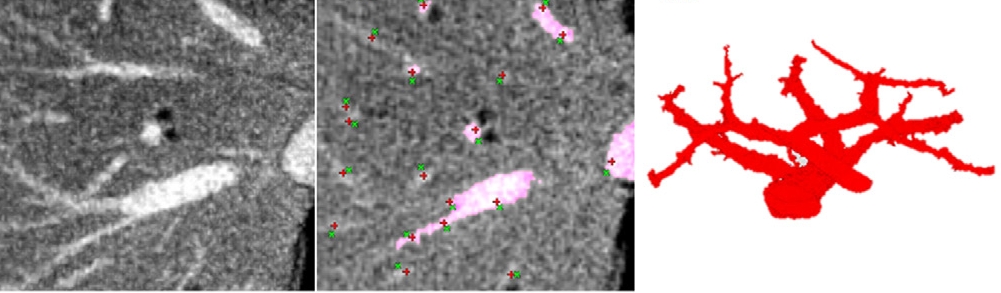
Quantitative evaluation of noise reduction and vesselness filters for liver vessel segmentation on abdominal CTA images Luu Manh Ha et al., PMB 2015 : Liver vessel segmentation in CTA images is a challenging task, especially in the case of noisy images. This study investigates whether pre-filtering improves liver vessel segmentation in 3D CTA images. We introduce a quantitative evaluation of several well-known filters based on a proposed liver vessel segmentation method on CTA images. We compare the effect of different diffusion techniques i.e. Regularized Perona–Malik, Hybrid Diffusion with Continuous Switch and Vessel Enhancing Diffusion as well as the vesselness approaches proposed by Sato, Frangi and Erdt. Liver vessel segmentation of the pre-processed images is performed using a histogram-based region grown with local maxima as seed points. Quantitative measurements (sensitivity, specificity and accuracy) are determined based on manual landmarks inside and outside the vessels, followed by T-tests for statistic comparisons on 51 clinical CTA images. The evaluation demonstrates that all the filters make liver vessel segmentation have a significantly higher accuracy than without using a filter (p < 0.05); Hybrid Diffusion with Continuous Switch achieves the best performance. Compared to the diffusion filters, vesselness filters have a greater sensitivity but less specificity. In addition, the proposed liver vessel segmentation method with pre-filtering is shown to perform robustly on a clinical dataset having a low contrast-to-noise of up to 3 (dB). The results indicate that the pre-filtering step significantly improves liver vessel segmentation on 3D CTA images.
An automatic registration method for pre- and post-interventional CT images for assessing treatment success in liver RFA treatment Luu Manh Ha et al., Med.Phys. 2015 In image-guided radio frequency ablation for liver cancer treatment, pre- and post-interventional CT images are typically used to verify the treatment success of the therapy. In current clinical practice, the tumor zone in the diagnostic, preinterventional images is mentally or manually mapped to the ablation zone in the post-interventional images to decide success of the treatment. However, liver deformation and differences in image quality as well as in texture of the ablation zone and the tumor area make the mental or manual registration a challenging task. Purpose of this study is to develop an automatic framework to register the pre-interventional image to the post-interventional image. To this end, we propose a registration approach enabling a nonrigid deformation of the tumor to the ablation zone, while keeping locally rigid deformation of the tumor area. The method was evaluated on CT images of 38 patient datasets from Erasmus MC. The evaluation is based on Dice coefficients of the liver segmentation on both the pre-interventional and post-interventional images, and mean distances between the liver segmentations. Additionally, residual distances after registration between corresponding landmarks and local mean surface distance in the images were computed. Results: The results show that rigid registration gives a Dice coefficient of 87.9%, a mean distance of the liver surfaces of 5.53 mm, and a landmark error of 5.38 mm, while non-rigid registration with local rigid deformation has a Dice coefficient of 92.2%, a mean distance between the liver segmentation boundaries near the tumor area of 3.83 mm, and a landmark error of 2.91 mm, where a part of this error can be attributed to the slice spacing in the authors’ CT images.
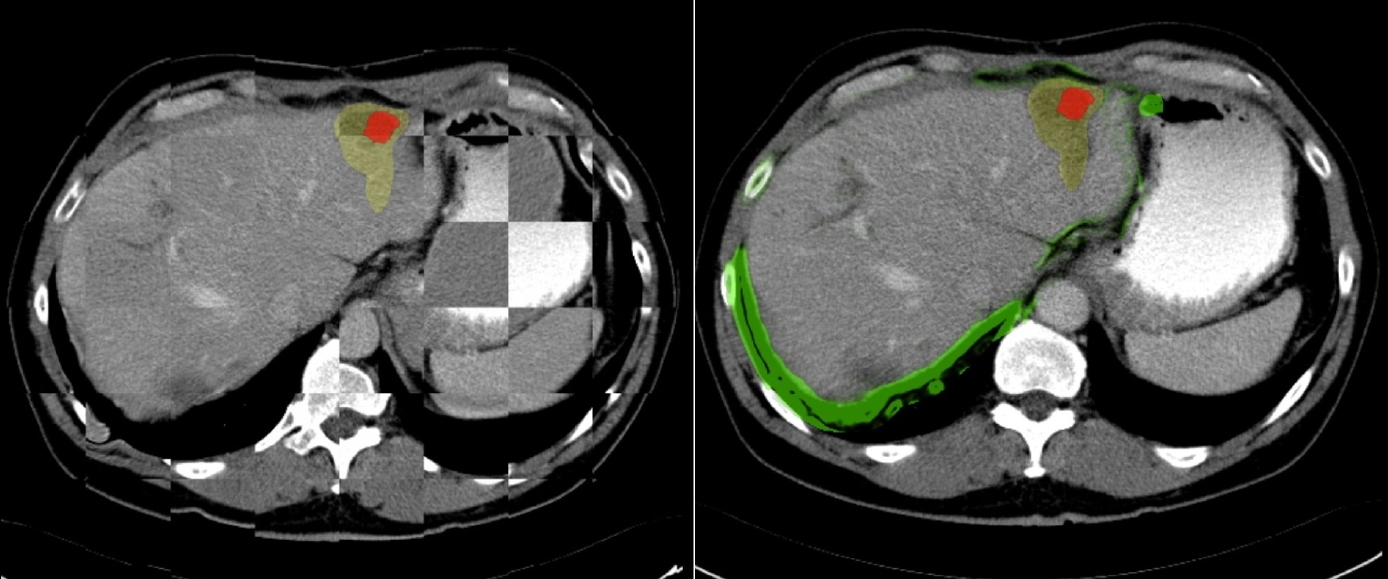
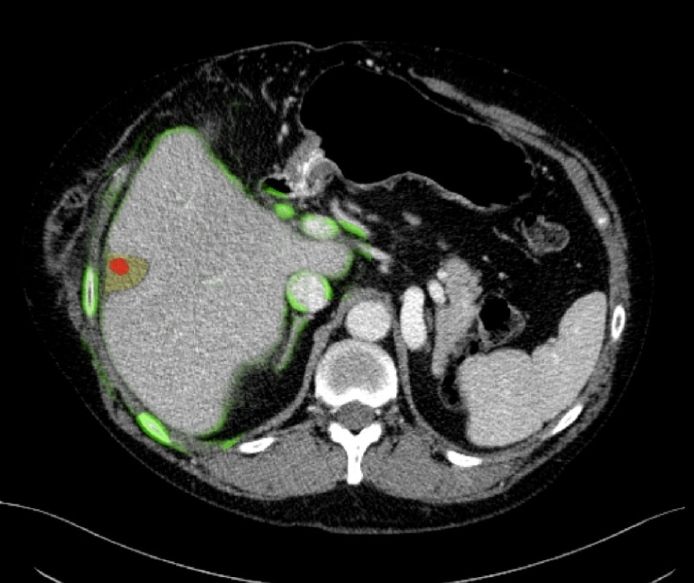
Non-Rigid Registration of Liver CT Images for CT-Guided Ablation of Liver Tumors Luu Manh Ha et al., Plos One 2016: CT-guided percutaneous ablation for liver cancer treatment is a relevant technique for patients not eligible for surgery and with tumors that are inconspicuous on US imaging. The lack of real-time imaging and the use of a limited amount of CT contrast agent make targeting the tumor with the needle challenging. In this study, we evaluate a registration framework that allows the integration of diagnostic pre-operative contrast enhanced CT images and intra-operative non-contrast enhanced CT images to improve image guidance in the intervention. The liver and tumor are segmented in the pre-operative contrast enhanced CT images. Next, the contrast enhanced image is registered to the intra-operative CT images in a two-stage approach. First, the contrast-enhanced diagnostic image is non-rigidly registered to a non-contrast enhanced image that is conventionally acquired at the start of the intervention. In case the initial registration is not sufficiently accurate, a refinement step is applied using non-rigid registration method with a local rigidity term. In the second stage, the intra-operative CT-images that are used to check the needle position, which often consist of only a few slices, are registered rigidly to the intra-operative image that was acquired at the start of the intervention. Subsequently, the diagnostic image is registered to the current intra-operative image, using both transformations, this allows the visualization of the tumor region extracted from pre-operative data in the intra-operative CT images containing needle. The method is evaluated on imaging data of 19 patients at the Erasmus MC. Quantitative evaluation is performed using the Dice metric, mean surface distance of the liver border and corresponding landmarks in the diagnostic and the intra-operative images. The registration of the diagnostic CT image to the initial intra-operative CT image did not require a refinement step in 13 cases. For those cases, the resulting registration had a Dice coefficient for the livers of 91.4%, a mean surface distance of 4.4 mmand a mean distance between corresponding landmarks of 4.7 mm. For the three cases with a refinement step, the registration result significantly improved (p<0.05) compared to the result of the initial non rigid registration method (DICE of 90.3% vs 71.3% and mean surface distance of 5.1 mmvs 11.3mmand mean distance between corresponding landmark of 6.4mmvs 10.2 mm). The registration of the preoperative data with the needle image in 16 cases yielded a DICE of 90.1% and a mean surface distance of 5.2 mm. The remaining three cases with DICE smaller than 80% were classified as unsuccessful registration.
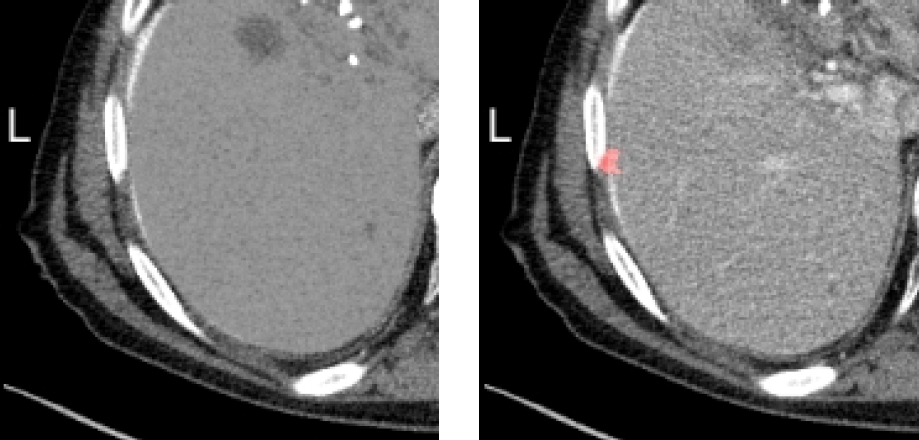
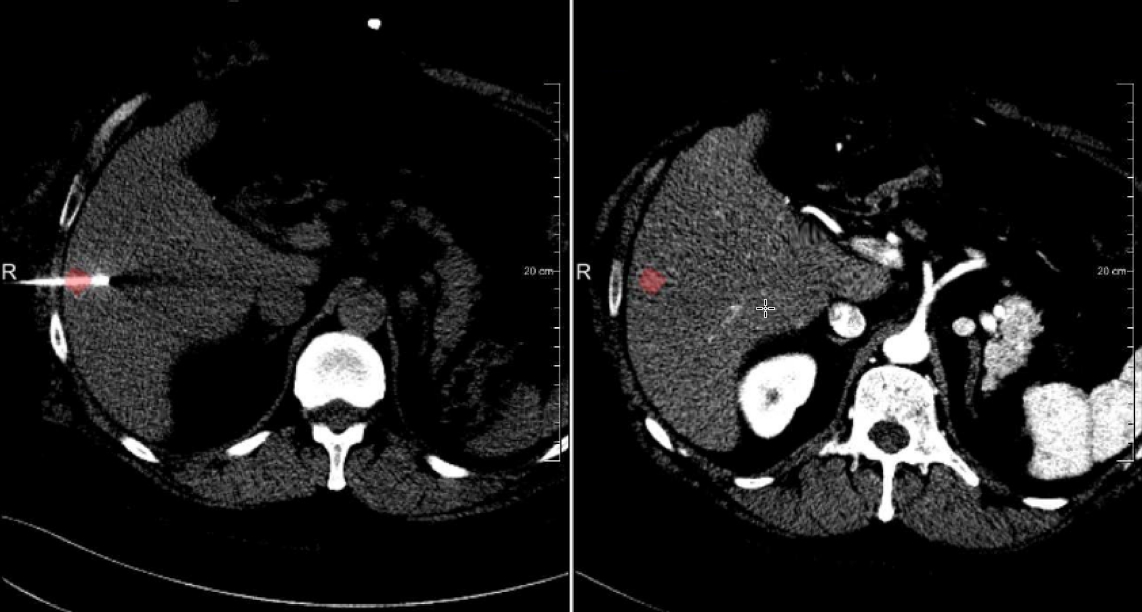
Luu Manh Ha et al., WBIR 2018: Image registration is relevant for many medical procedures. For CT-guided ablation procedures, integrating the lesion location from diagnostic contrast-enhanced CT (CECT) images in interventional CT images may provide better guidance for the interventional radiologist. The main requirement for such methods is to accurately align the lesion location. This, in general, can not be measured, and often surrogates are used for the assessment. In this work, we present a method that permits the assessment of the accuracy of the lesion localization, i.e. assessing the value that is relevant for clinical practice. To this end, we developed a method that virtually removes the contrast agent from an interventional CT image, use this image for the registration, and use the original CECT image for the assessment. For the experimental evaluation, imaging data of 20 subjects (33 lesions) were used, and the registration accuracy of a publicly available registration method was assessed using this method.
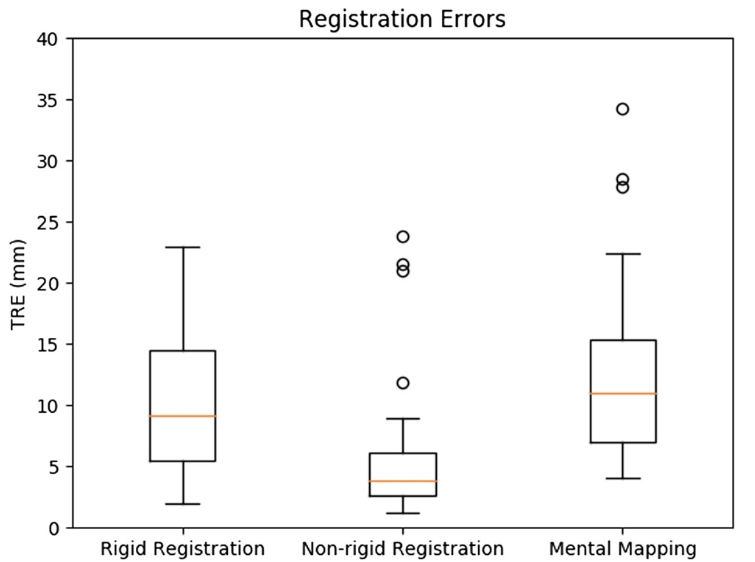
Accuracy of semi-automated versus manual localisation of liver tumours in CT-guided ablation procedures Boulkhrif et al., European Radiology 2018: The registration was also compared to human observers. To this end, 35 contrast-enhanced CT (CECT) images incorporating 56 tumours, acquired during CTguided ablation procedures and their corresponding pre-procedural diagnostic CECTs were retrieved from the picture archiving and communication system (PACS). The original intraprocedural CECTs were de-enhanced to create a virtually unenhanced CT image (VUCT). Alignment of diagnostic CECTs to their corresponding intraprocedural VUCTs was performed with non-rigid or rigid registration. Mental registration was performed by four interventional radiologists. The original intraprocedural CECT served as the reference standard. Accuracy of tumour localisation was assessed with the target registration error (TRE). Statistical differences were analysed with the Wilcoxon signed-rank test. The non-rigid registration failed to register two CT datasets, incorporating four tumours. In the remaining 33 datasets, nonrigid, rigid and mental registration showed a median TRE of 3.9 mm, 9.0 mm and 10.9 mm, respectively. Non-rigid registration was significantly more accurate in tumour centre localisation in comparison to rigid (p <0.001)ormentalregistration(p <0.001). Rigid registration was not statistically different from mental registration (p = 0.169). Non-rigid registration was most accurate in localising tumour centres in 42 out of 52 tumours (80.8%), while rigid and mental registration were most accurate in only seven (13.5%) and three (5.8%) tumours, respectively. We conclude that computer-based non-rigid registration is statistically significantly more accurate in localising liver tumours in intraprocedural unenhanced CT images in comparison to rigid registration or interventional radiologists’ mental mapping abilities.


